For immediate answers to questions, please go to https://www.realself.com/find/California/Beverly-Hills/Plastic-Surgeon/Charles-Lee#qa
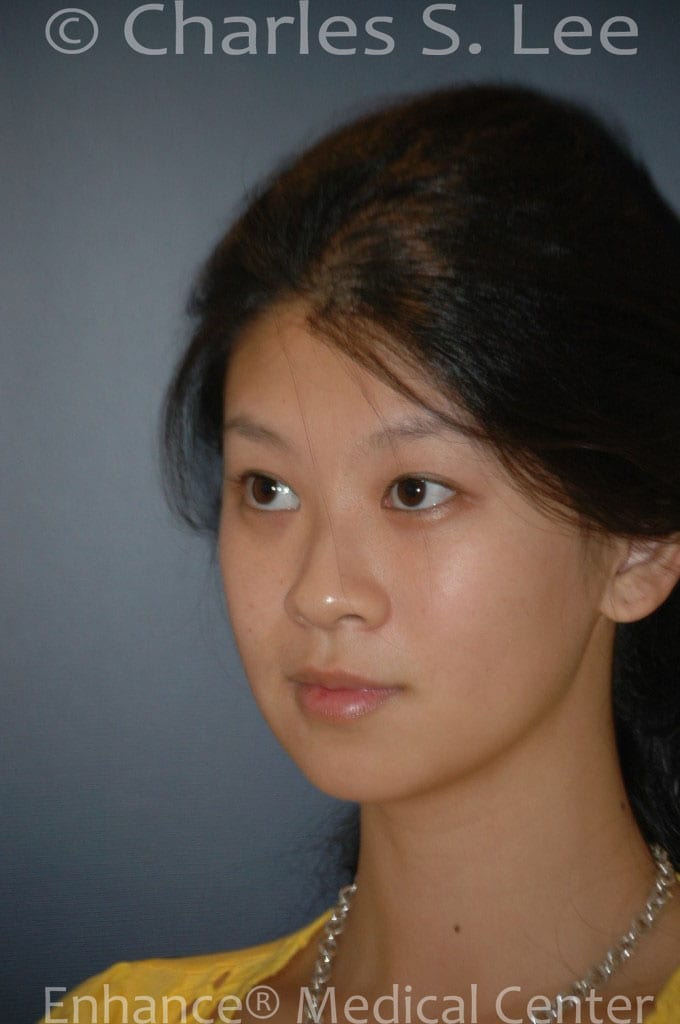
Asian eyelid surgery, asian nose surgery, chin implant and buccal fat removal. This patient had several plastic surgery procedures common among Asians. Asian eyelid surgery, or asian double eyelid surgery, asian rhinoplasty or asian nose surgery, as well as buccal or cheek fat removal and chin implant.
Asian eyelid surgery, asian nose surgery, chin implant and buccal fat removal
The details of this procedure will be outlined below. For nasal surgery, the author prefers silastic or gortex nasal implants for the bridge and cartilage to the tip area, and nostril narrowing as needed. We prefer closed rhinoplasty, with no external cuts. All natural tissue can be used if desired by the patient.
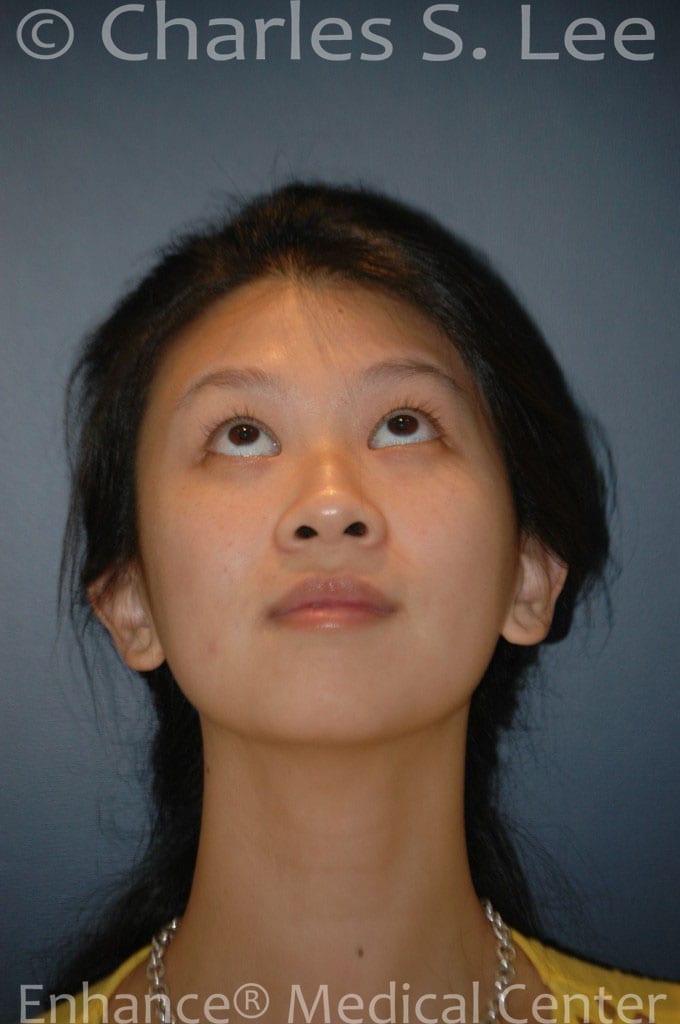
This patient had an uneven nose bridge, especially between the eyes, and the tip of the nose was low. Also, the nostrils were wide. The nose was corrected with a nose implant (silicone or silastic) implant, and the tip was made stronger with additional cartilage taken from elsewhere.
The chubbiness of the cheeks were corrected by removing fat from the cheeks, also known as buccal fat.






How the surgery was performed:
Analysis of the nose: the preoperative nose is noticeable for the depression at the root of the nose, between the eyes. The middle portion of the nose has adequate height. The tip of the nose, referred as the bottom third, is notable for the roundness and lack of strength. The nostrils are slightly wide and flared.
The chin is slightly weak.
There is slight fullness to the cheek area.
Overall, the patient has very attractive features which would be improved dramatically with relatively small enhancements.
The surgical details:
The bridge: this area can be straightened by using natural tissue or silastic/ gortex implants. We prefer the silastic/gortex materials as a first choice in patients who have had either no or only one prior surgery. The shape of the implant is made much more smoothly and evenly than possible with handmade natural materials. Thus, silicone is our default material of choice. FDA approved silastic implants have withstood the test of time and do not need to be changed periodically.
Our patient’s bridge was remarkable for the extra thickness need at the area between the eyes, which necessitated careful carving of the implant. Using a straight piece of implant would have required too much removal of her native tissue. Alternatively, natural tissue could have been placed between the eyes to raise it in alignment with the rest of the bridge. In our experience, it is more straightforward to place a silastic implant.
The tip of the nose was addressed by strenghthening the cartilage of the bottom third of the nose, the tip area. Characteristic of Asian noses, and up to 50{0fd4121d5216b280473771676d11ae34909381d9377f36f96353e02149c70f16} of Caucasian noses, the cartilage of the tip of the nose is weak and does not support the tip skin. The resulting roundness of the tip is made more attractive by reinforcing the weak nasal tip cartilage, by buttressing it, similar to a tent pole holding up the top of the dome. This requires a rigid piece of cartilage.
This bottom third of the nose can be round, or “bulbous” in Caucasian noses as well. In the Caucasian nose, the roundness is typically caused by overgrowth of the cartilage. The correction for this condition is removal of the overgrown cartilage.
In Asian noses, however, the cause of the roundness is not overgrowth of tissue, but rather the weakness of the cartilage. In inexperienced hands, it is common to remove cartilage from the Asian nose in an attempt to correct the roundness of the tip. However, this will invariably result in a worsening of the condition, since the cause of the roundness of the nasal tip is completely opposite between Caucasian and Asian noses.
Instead, the tip of the Asian nose must be reinforced and strengthened. The ideal cartilage is the septum, which is the tissue inside the nose, which separates the two nostrils (and prevents one’s finger from entering one nostril and exiting the other). This tissue, if strong enough, can give the support to the nasal tip that can give an ideal result. The septum is usable for Asian rhinoplasty in about 50{0fd4121d5216b280473771676d11ae34909381d9377f36f96353e02149c70f16} of cases. This typically is usable in Asians from northeastern Asia.
In patients from southern Asia, the septal cartilage is often insufficient in strength and quantity to give adequate tip support. In such cases, the cartilage from behind the ear can be used instead. The primary drawback to this tissue is that the ear cartilage shape is irregular, and placing it along the tip of the nose can result in visible irregularities of the tip.
The main other source of cartilage for the tip is from the rib, either the patient’s own, or from a donated tissue bank, tested for viruses and irradiated. Circulation to the tip must be maintained in order to minimize resorption, thus the preference our center places on the closed rhinoplasty procedure.
The nostrils are addressed in order to both narrow their width, as well as to improve their shape (the latter referred to as “flare”). Internal incisions are employed to narrowed Caucasian noses after reducing the tip height (popularized by D. R Millard after his presentation in the 1950). In Asian, a more classic removal of a crescent of skin, or an external “Weir” incision is preferred (named for Dr. Robert Weir, the inventor of the procedure in the 1890’s). The incision is made in the groove where the nostril meets the cheek. The incision heal without much visibility over the course of several months to a year.
The chin implant is placed to improve the overall balance to the face after the nasal surgery has been performed. The incision can be made either from inside the mouth or externally, from a small incision in the skin of the chin. We prefer the internal incision whenever possible, as popularized by D. R. Millard, also in the 1950’s.
Buccal fat is the cheek fat that gives a youthful appearance to the face. This fat shrinks with aging. We prefer not to remove this fat except in patients whose family history shows persistence of fat despite the aging process. These patients show prominent cheeks beyond their mid-30’s. Parents often exhibit such tendencies, and in such cases, we will remove the cheek fat through internal incisions. The result is a more sophisticated, oval face in the appropriate patient.
The patient above was presentable at the 7 day mark. All sutures were removed at that point, and she returned to social interaction. By two to three weeks, very little evidence of surgery is seen.






{kind=link}
{kind=link}
{kind=link}